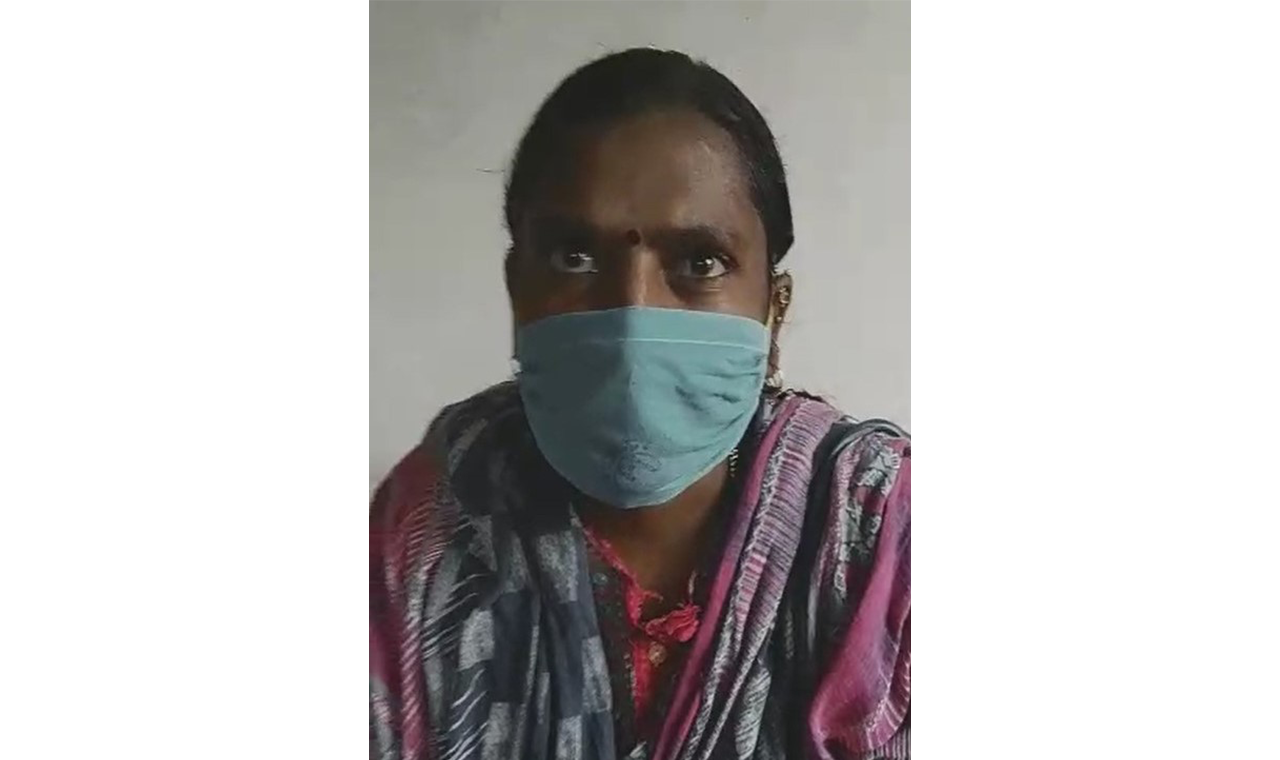
Bio-behavioural surveys confirm that HIV prevalence is high or ‘concentrated’ among ‘key populations’ (KPs) who have unprotected sexual contacts with multiple partners or who engage in injecting drug use. These populations include female sex workers (FSW), men who have sex with men (MSM), hijra/transgender (TG), people who inject drugs (PWID), long-distance truck drivers and migrants and HIV disproportionately affects these people. Stigma and discrimination persist everywhere and continue to prevent HIV services from reaching the people who need them most. In addition, young women at childbearing age are also at higher risk of infection and the source of onward transmission to their infants, during birth, labour and through breastfeeding.
Our Approach
Our HIV programmes focus on rapid scaling of prevention, care, and support programmes.
Peer-led intervention Model
Peer education interventions are adopted as a strategy for preventing HIV and other sexually transmitted infections (STIs) among key populations. Peer education programs are based on the rationale that peers have a strong influence on individual behaviour. As members of the target group, peer educators are assumed to have a level of trust and comfort with their peers that allows for more open discussions of sensitive topics. Similarly, peer educators are thought to have good access to hidden populations that may have limited interaction with more traditional health programs.
Risk and Vulnerability Reduction approach
Risk reduction strategies include community-led outreach and behaviour change communications that is differentiated and responsive to community needs; ensuring access to correct knowledge about STI and HIV among female sex workers, men who have sex with men, hijras and their regular partners; negotiation skills for sexual encounters; ensuring access to services for STI and other health problems; promoting male and female condoms; and creating safe spaces.
Vulnerability reduction strategies include developing crisis response systems; advocating with key influencers in the sex work circuit and government including sensitising police about violence against the key population; facilitating access to rights and entitlements through the provision of basic social entitlements and welfare supports such as ration card, children’s education, reducing economic dependence on sex work; and building community ownership through the participation of the key population in the project.
Community Mobilization and Empowering the community through Collectivisation
Community mobilisation is purposefully steered towards the formation of groups or collectives and capacity building of the key population. This enables a larger role for the community-based organisations, prepares them to eventually assume responsibility for the issues that affect them, and empowers them as the natural owners of HIV programs.
Our Achievements
We have won numerous awards including BMGF –AVAHAN Awards, awarded in 2013
> In recognition of Community transition: Successful transfer of CBOs to the government while maintaining quality and community ownership
> In recognition of Institutional building of MARP communities –forming community groups for social cohesion and identity
> In recognition of programmatic innovation to increase accessibility and availability of services and their utilization for MARPs
> In recognition of Resource mobilisation through community events and stakeholder engagement to bring visibility to communities
> In recognition of Advocating and facilitating linkages with government schemes for communities.
Our innovative models have been nationally and globally scaled up, including
> KP intervention models – micro-planning, community mobilisation, peer education
> STI management – colour-coded medicines and private provide engagement
> Rural intervention for HIV prevention (Link Workers Scheme)
> Prevention of Parent to Child Transmission (PPTCT) program